
Trends in Oncology
The Complex Case of Hepatocellular Carcinoma Clinical Management
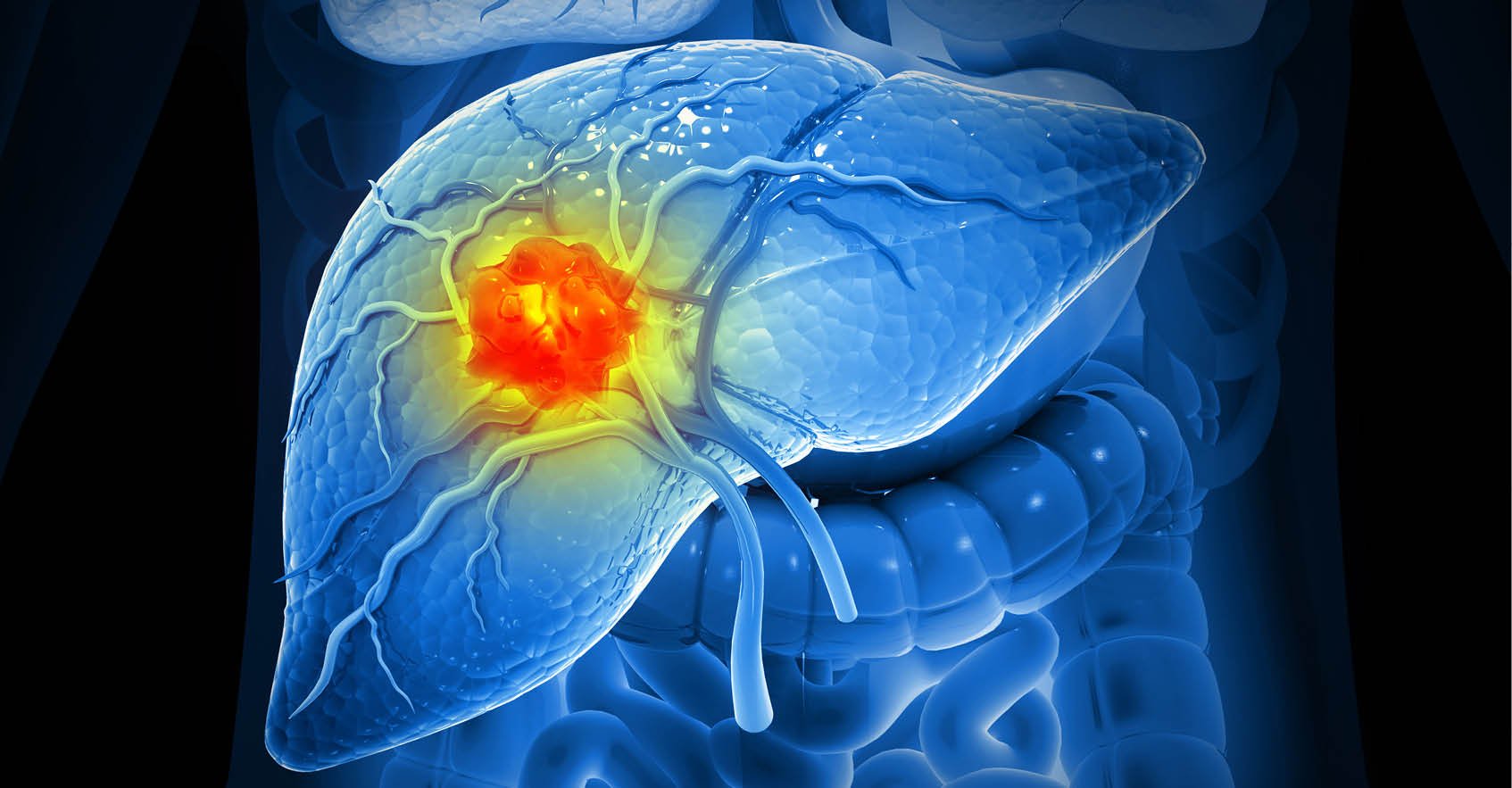
Hepatocellular carcinoma (HCC) is one of the most prevalent types of liver cancer, and it usually develops in patients with underlying cirrhosis or chronic liver disease and metabolic syndrome.[1] HCC can spread to other body parts and affect patients' survival rates and outcomes severely. In this blog post, we will provide essential insights into HCC metastases and delve into the therapeutic options. Over 60% of patients with HCC are diagnosed in advanced stages, leading to an overall 5-year survival rate of 21%. However, this rate is between 60% and 70% in patients with early diagnosis who undergo liver transplants.[2] Patients diagnosed with advanced-stage HCC, defined by the presence of vascular invasion or extrahepatic metastases, have a poor prognosis with a median survival of less than 1 year. [3] Early detection of HCC is vital in increasing therapeutic opportunities and improving patients’ outcomes, and new diagnostic biomarkers are under investigation to enhance HCC screening.[4] Available treatments for HCC metastases depend on the tumor's location, the extent of the cancer, and the patient's general condition. Surgical resection, liver transplant, radiofrequency, and microwave ablation are all first-line treatments for tumors that have not spread to other body parts. Chemoembolization is commonly used and improves survival in asymptomatic patients with multifocal regional disease. [5] Systemic therapies, such as sorafenib and lenvatinib have been shown to be effective in prolonging survival rates and outcomes in patients with advanced HCC. These agents are multikinase inhibitors that block tyrosine kinases involved in angiogenesis, cancer development and growth, and tumor microenvironment regulation. They are used as first-line therapy in advanced HCC with contraindications to VEGF and immune checkpoint inhibitors. Immune checkpoint inhibitors are instead used together with bevacizumab in patients without contraindication. Alternative tyrosine kinase inhibitors, such as regorafenib, cabozantinib, and ramucirumab are used as second-line treatments.[6] Scientists are also researching new therapies for advanced HCC, including novel molecular-targeted therapies (such as STAT3 and CDK4 inhibitors) and immunotherapies to use as single agents or in combination. Several clinical trials are currently underway to investigate the efficacy and safety of these new therapies for advanced and metastatic HCC.[7] Hepatocellular carcinoma is a critical concern for clinicians and patients, given the cancer progression and severity. Validating new diagnostic biomarkers and developing new therapeutic approaches to overcome drug resistance will be paramount in improving patients’ survival and quality of life.
Hitting the Target: Latest Developments in Anti-Her2 Therapy
Human epidermal growth factor receptor 2 (HER2; ERBB2) has been shown to induce oncogenesis in several cancers, particularly breast and gastric cancers. HER2 is estimated to be overexpressed in ~20% of all breast cancers, and outcomes for these breast cancers were poor before HER2-targeted therapies[1]. Our understanding of mechanisms by which HER2 drives tumor growth and metastasis led to one of the first targeted therapies for treating HER2+ breast cancers. Here we highlight what is known about HER2 and oncogenesis. and how this information can be applied to the development of new targeted therapies. Gene amplification of the ERRB2 oncogene is one of the most common genetic defects detected in HER2+ tumors and typically causes overexpression of HER2 at the cell membrane[2]. HER2 proteins more readily dimerize with other HER2 proteins to form homodimers or with other ERRB members to form heterodimers. These complexes induce oncogenic signaling cascades, including MAPK and PI3K/AKT/mTOR, which cause cellular proliferation, angiogenesis, and resistance to apoptosis[3]. Due to the dominant role of HER2 in breast cancer, anti-HER2 antibodies were developed as one of the first targeted therapies. In 2006, clinical trial results of breast cancer patients treated with the anti-HER2 antibody trastuzumab showed significant improvements in progression-free survival and overall survival[4],[5]. Unfortunately, ~20-25% of metastatic breast cancer patients develop resistance to anti-HER2 therapies. More recent studies have focused on engineering new forms of anti-HER2 antibodies or developing HER1/2 inhibitors that can be used alone or in combination with other targeted therapies. The current standard of care for HER2+ breast cancer includes chemotherapy with adjuvant HER2-targeted therapies and endocrine therapy as indicated. Advances in targeted therapies are further improving treatment protocols. The next-generation anti-HER2 monoclonal antibody margetuximab targets the same HER2 epitope as trastuzumab and is modified in its Fc domain to improve antibody-dependent cellular cytotoxicity.[6] Margetuximab was approved by the FDA in December 2020 for the treatment of metastatic breast cancer in patients who had received prior HER2 therapies[7]. Two different bispecific antibodies have also been developed and are in clinical trials: ZW25 is a bispecific antibody that targets two different HER2 epitopes, and PRS-343 is a bispecific antibody that targets a HER2 epitope and the 4-1BB costimulatory immunoreceptor[8]. Bispecific antibodies are under development for breast cancer and other cancers because they exploit the property that antibodies have two epitope binding sites and can be engineered to better target a single molecule or crosslink multiple molecules, like HER2 and immune checkpoint molecules. Antibody-drug conjugates have also been evaluated as novel therapeutics that target HER2. Trastuzumab deruxtecan is an anti-HER2 antibody conjugated to a cytotoxic payload that is linked by a cleavable drug linker[9]. This treatment has been recently approved by the FDA and it shows superior targeting of cytotoxic drugs to HER2+ tumor cells and shows efficacy on individuals who have been treated previously with anti-HER2 mAbs. HER2-specific tyrosine kinase inhibitors have also been successful in treating HER2+ tumors, especially brain metastases because these drugs can cross the blood-brain barrier. Lapatinib, neratinib, pyrotinib, and tucatinib are four HER2-specific tyrosine kinase inhibitors used to treat HER2+ breast cancers. Lapatinib is an oral, irreversible small molecule HER1/HER2/HER4 TKI that was first approved in 2007 for the treatment of metastatic breast cancer[10]. Neratinib is a similar, orally available irreversible small molecule HER1/HER2/HER4 TKI that showed better efficacy against EGFR mutants and has been approved for use as an adjuvant therapy following trastuzumab treatment[11]. The development of resistance is also a problem for HER2-targeted TKIs, and pyrotinib is an experimental HER1/HER2/HER4 TKI under investigation as a potential new drug that is less prone to resistance[12]. Tucatinib is a TKI that is highly selective for HER2 approved for use in combination with trastuzumab and capecitabine in HER2+ breast and colorectal cancers, including patients with metastases and who have received previous anti-HER2 treatment[13]. HER2+ breast cancers continue to be challenging to treat due to resistance and metastasis. Combination therapies with antibodies and targeted inhibitors have dramatically improved survival in HER2+ breast cancer patients, but individuals who relapse continue to be faced with limited treatment options. New antibody-drug conjugates, bispecific antibodies, and targeted inhibitors are under investigation and hold the promise of better, more durable treatment options for patients. [1] Hudis CA. Trastuzumab--mechanism of action and use in clinical practice. N. Engl. J. Med. 2007 Jul 5;357(1):39-51. [2] Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987 Jan 9;235(4785):177-82. [3] Moasser MM. The oncogene HER2: its signaling and transforming functions and its role in human cancer pathogenesis. Oncogene. 2007 Oct 4;26(45):6469-87. [4] Romond EH, Perez EA, Bryant J, Suman VJ, Geyer Jr CE, Davidson NE, Tan-Chiu E, Martino S, Paik S, Kaufman PA, Swain SM. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N. Engl. J. Med. 2005 Oct 20;353(16):1673-84. [5] Smith I, Procter M, Gelber RD, Guillaume S, Feyereislova A, Dowsett M, Goldhirsch A, Untch M, Mariani G, Baselga J, Kaufmann M. 2-year follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer: a randomised controlled trial. Lancet. 2007 Jan 6;369(9555):29-36. [6] Rugo HS, Im SA, Cardoso F, Cortés J, Curigliano G, Musolino A, Pegram MD, Wright GS, Saura C, Escrivá-de-Romaní S, De Laurentiis M. Efficacy of margetuximab vs trastuzumab in patients with pretreated ERBB2-positive advanced breast cancer: a phase 3 randomized clinical trial. JAMA Oncol. 2021 Apr 1;7(4):573-84 [7] https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-margetuximab-metastatic-her2-positive-breast-cancer. [8] Kunte S, Abraham J, Montero AJ. Novel HER2-targeted therapies for HER2-positive metastatic breast cancer. Cancer. 2020 Oct 1;126(19):4278-4288. [9] Doi T, Shitara K, Naito Y, Shimomura A, Fujiwara Y, Yonemori K, Shimizu C, Shimoi T, Kuboki Y, Matsubara N, Kitano A, Jikoh T, Lee C, Fujisaki Y, Ogitani Y, Yver A, Tamura K. Safety, pharmacokinetics, and antitumour activity of trastuzumab deruxtecan (DS-8201), a HER2-targeting antibody-drug conjugate, in patients with advanced breast and gastric or gastro-oesophageal tumours: a phase 1 dose-escalation study. Lancet Oncol. 2017 Nov;18(11):1512-1522. [10] Ryan Q, Ibrahim A, Cohen MH, Johnson J, Ko CW, Sridhara R, Justice R, Pazdur R. FDA drug approval summary: lapatinib in combination with capecitabine for previously treated metastatic breast cancer that overexpresses HER-2. Oncologist. 2008 Oct;13(10):1114-9. [11] Minami Y, Shimamura T, Shah K, LaFramboise T, Glatt KA, Liniker E, Borgman CL, Haringsma HJ, Feng W, Weir BA, Lowell AM, Lee JC, Wolf J, Shapiro GI, Wong KK, Meyerson M, Thomas RK. The major lung cancer-derived mutants of ERBB2 are oncogenic and are associated with sensitivity to the irreversible EGFR/ERBB2 inhibitor HKI-272. Oncogene. 2007 Jul 26;26(34):5023-7. [12] Li Q, Guan X, Chen S, Yi Z, Lan B, Xing P, Fan Y, Wang J, Luo Y, Yuan P, Cai R, Zhang P, Li Q, Zhong D, Zhang Y, Zou J, Zhu X, Ma F, Xu B. Safety, Efficacy, and Biomarker Analysis of Pyrotinib in Combination with Capecitabine in HER2-Positive Metastatic Breast Cancer Patients: A Phase I Clinical Trial. Clin. Cancer Res. 2019 Sep 1;25(17):5212-5220. [13] Murthy RK, Loi S, Okines A, Paplomata E, Hamilton E, Hurvitz SA, Lin NU, Borges V, Abramson V, Anders C, Bedard PL, Oliveira M, Jakobsen E, Bachelot T, Shachar SS, Müller V, Braga S, Duhoux FP, Greil R, Cameron D, Carey LA, Curigliano G, Gelmon K, Hortobagyi G, Krop I, Loibl S, Pegram M, Slamon D, Palanca-Wessels MC, Walker L, Feng W, Winer EP. Tucatinib, Trastuzumab, and Capecitabine for HER2-Positive Metastatic Breast Cancer. N Engl J Med. 2020 Feb 13;382(7):597-609.
Prostate Cancer - Drivers of Genetic Mutations & Their Role in Disease Progression
Prostate cancer is one of the most common forms of cancer that affects the prostate gland in the male urogenital tract. Most prostate cancers are slow growing and are usually detected in individuals older than age 50. Although environmental factors contribute to the development of prostate cancer, risk is significantly associated with incidence among first-degree relatives. In recent years, several inherited and spontaneously mutated genes have been linked to prostate cancer. Here we highlight these findings and how they provide insight into the development of targeted prostate cancer therapies. Prostate cancer tumors are typically characterized by a wide range of genomic aberrations including somatic copy number alterations (SCNAs), structural rearrangements, and point mutations. Metastatic prostate tumors may have hundreds of these aberrations throughout the genome, but recent studies of primary prostate tumors have been critical to defining mutations associated with tumor development. Most primary prostate tumors have SCNAs, typically in the form of deletions that target a small area of the genome1. Deletions are often seen in the tumor suppressor genes BRCA2, NKX3.1, PTEN, and RB12. Structural rearrangements are another source of genomic variation observed in primary prostate tumors, for which the TMPRSS2:ERG rearrangement is most common and causes the androgen-responsive TMPRSS2 serine protease to drive expression of the ERG oncogene3. Other rearrangements have been linked to prostate cancer, including TMPRSS2 fusions with other ETS family members beyond ERG (ETV1 and ETV4)4. Some studies have suggested a link between ERG rearrangements and SCNA incidence, although it is not yet clear if rearrangements lead to destabilization of the genome and increased occurrence of SCNAs1. Somatic mutations occur on relatively high frequency primary prostate tumors, and this has been linked to mutations DNA mismatch repair proteins, tumor suppressors and oncogenes. The tumor suppressor TP53 is consistently identified as mutated in prostate tumors5. Mutations in the tumor suppressor genes BRCA1 and BRCA2 are well known for their association with breast and ovarian cancer but have also been linked to prostate cancer, and recent studies have shown that certain BRCA2 pathogenic sequence variants are associated with an elevated risk for aggressive prostate cancer6,7. PALB2 is a protein that interacts with BRCA2, and a recent study indicated that individuals who have certain PALB2 variants are more predisposed to aggressive forms of prostate cancer8. In addition, mutations in genes associated with DNA mismatch repair (MMR), such as MSH2, MSH6, and MLH1, are associated with greater prostate cancer risk9, and individuals with Lynch syndrome, which is caused by a germline mutation in one of these MMR genes, are also at greater risk of developing an aggressive form of prostate cancer10. One of the most important genes involved in prostate cancer progress is the gene expressing the androgen receptor (AR). Dozens of somatic mutations have been identified in the AR, and many of these mutations target the ligand binding domain11. Some prostate cancers can be treated successfully with drugs that inhibit AR signaling, such as enzalutamide, but resistance frequently occurs and is associated with worse outcomes. AR promotes prostate cancer cell survival by regulating several cellular programs. Although AR activity inhibition through androgen deprivation therapy (ADT) results in the suppression of AR-related pathways and durable clinical remission12, the disease may recur as castration-resistant prostate cancer (CRPC), typically with reactivated AR signaling. In this case, patients are treated with second-generation AR pathway inhibitors such as enzalutamide and abiraterone. Unfortunately, durable complete responses under these treatments are rare, and a substantial number of CRPC tumors progress under treatment despite loss of AR signaling. CRPC with AR-null phenotype are classified as tumors with diffuse small cell or neuroendocrine (NE) characteristics (SCNPC) or as double-negative (DNPC) phenotype that lacks both NE and AR activity13. A recently described genome-wide CRISPR-Cas9 screen was used to identify kinases that could be inhibited in the presence of enzalutamide. BRAF or downstream MAPK signaling molecules were identified as targets that could be co-inhibited with enzalutamide to improve overall therapeutic effects of these drugs14. Genomic alterations in prostate cancer are highly variable and can impact many critical cellular processes. By understanding which genes drive disease progression, potential therapeutic targets can be identified, and disease outcomes under different treatment regimens can be better predicted. [1] Taylor BS, Schultz N, Hieronymus H, et al. Integrative genomic profiling of human prostate cancer. Cancer Cell. 2010 Jul 13;18(1):11-22. [2] Wallis CJ, Nam RK. Prostate Cancer Genetics: A Review. EJIFCC. 2015 Mar 10;26(2):79-91. [3] Tomlins SA, Rhodes DR, Perner S et al. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science. 2005 Oct 28;310(5748):644-8. [4] Rubin MA, Maher CA, Chinnaiyan AM. Common gene rearrangements in prostate cancer. J. Clin. Oncol. 2011 Sep 20;29(27):3659-68. [5] Ecke TH, Schlechte HH, Schiemenz K et al. TP53 gene mutations in prostate cancer progression. Anticancer Res. 2010 May 1;30(5):1579-86. [6] Patel VL, Busch EL, Friebel TM, et al. Association of Genomic Domains in BRCA1 and BRCA2 with Prostate Cancer Risk and Aggressiveness. Cancer Res. 2020 Feb 1;80(3):624-638. [7] Oh M, Alkhushaym N, Fallatah S, et al. The association of BRCA1 and BRCA2 mutations with prostate cancer risk, frequency, and mortality: A meta-analysis. Prostate. 2019 Jun;79(8):880-895. [8] Wokołorczyk D, Kluźniak W, Stempa K, Rusak B, Huzarski T, Gronwald J, Gliniewicz K, Kashyap A, Morawska S, Dębniak T, Jakubowska A. PALB2 mutations and prostate cancer risk and survival. Br. J. Cancer. 2021 May 18:1-7. [9] Ritch E, Fu SY, Herberts C, Wang G, et al. Identification of hypermutation and defective mismatch repair in ctDNA from metastatic prostate cancer. Clin. Cancer Res. 2020 Mar 1;26(5):1114-25. [10] Haraldsdottir S, Hampel H, Wei L, et al. Prostate cancer incidence in males with Lynch syndrome. Genet. Med. 2014 Jul;16(7):553-7. [11] Ferraldeschi R, Welti J, Luo J, Attard G, de Bono JS. Targeting the androgen receptor pathway in castration-resistant prostate cancer: progresses and prospects. Oncogene. 2015 Apr 2;34(14):1745-57. [12] Heinlein CA, Chang C. Androgen receptor in prostate cancer. Endocr Rev. 2004;25(2):276–308. [13] Bluemn EG, Coleman IM, Lucas JM et al. Androgen receptor pathway-independent prostate cancer is sustained through FGF signaling. Cancer Cell. 2017;32(4):474–489. [14] Palit SAL, van Dorp J, Vis D, Lieftink C, Linder S, Beijersbergen R, Bergman AM, Zwart W, van der Heijden MS. A kinome-centered CRISPR-Cas9 screen identifies activated BRAF to modulate enzalutamide resistance with potential therapeutic implications in BRAF-mutated prostate cancer. Sci. Rep. 2021 Jul 1;11(1):13683. Subscribe to our Trends in Oncology Blog
ERK at Work - Targeting the ERK Pathway in Cancer
Signal transduction networks are essential to normal cell growth and function, but signaling abnormalities, such as those caused by spontaneous mutations in signaling components, are the leading causes of tumor growth. The extracellular signal-regulated kinase (ERK) signaling pathway contributes to normal cell proliferation, differentiation, and survival, but components of the ERK pathway are upregulated in many tumor types, including those associated with melanoma, lung, colon and pancreatic cancers. The critical role of the ERK pathway in cancer has resulted in the development of drugs and therapeutics that can inhibit overactivation of ERK signaling molecules or target aberrant signaling pathways upstream of ERK. The emergence of precision medicine-driven cancer treatments has advanced the ERK pathway inhibitor field. Breakthroughs in cancer genomics has enabled researchers to analyze tumor sequences derived from patient data and identify novel targets in the ERK pathway. This type of computational analysis coupled with large scale in vitro screening is essential to narrowing down which novel inhibitors are studied further during preclinical development. The use of patient-derived xenograft (PDX) mouse models is critical to the discovery of next-generation ERK inhibitors. PDX models involve the use of mice that are engrafted with tumor tissue derived from patient samples. These mice typically have suppressed immune systems in order to tolerate tumor grafts and can be engineered to express other components of the human immune system, such as immune checkpoint inhibitors. PDX models that use tumors with mutations in ERK signaling, such as a colorectal tumor with a V600-mutated BRAF molecule, can be used in the preclinical screening of novel ERK pathway inhibitors. Novel inhibitors can be screened simultaneously in different PDX models, and the safety and efficacy of these molecules can also be assessed in combination with other therapeutics. We are entering an era when cancer patients will have access to precision medicine treatments informed by the genetic analysis of their tumors, and the strategic deployment of new and improved ERK pathway inhibitors in patients with specific ERK mutations will improve treatment efficacy and overall survival. PDX models are essential to the development of these new ERK pathway inhibitors and many other novel immunotherapies.
Sarcoma Immunotherapeutic Strategies
Sarcomas are a group of aggressive heterogeneous tumors for which more than 100 histological subtypes have been defined1. Sarcomas are found in a variety of solid tissues, including bone and gastrointestinal stromal cells. Current treatment options include radiotherapy, surgical resection, targeted therapies, and chemotherapy, but these treatments have had limited efficacy on intermediate to high-grade tumors. Investigations into the molecular and cellular mechanisms that drive sarcomas have helped identify potential biomarkers that can serve as potential therapeutic targets. In addition, recent studies have also focused on the tumor microenvironment (TME) within sarcomas and the roles of different immune cell subsets creating an immunosuppressive microenvironment. These observations directly inform novel immunotherapeutic approaches that are being examined in preclinical and clinical studies. Sarcoma TME and Immune Checkpoint Blockade In general, sarcoma TMEs are highly immunosuppressive environments, and a recent analysis of the Ewing’s sarcoma family of tumors (ESFT) showed poor overall survival correlated with tumors that had a TME with elevated expression of hypoxia-inducible factor 1-α and were enriched with immunosuppressive M2 macrophages and neutrophils2. The presence of tumor-associated macrophages has also been linked to sarcoma growth and metastasis, and elevated expression of the immune checkpoint molecule PD-L1 also correlated with metastasis and poor overall survival3,4. These observations led to clinical trials that evaluated the efficacy of immune checkpoint blockade for treating sarcomas, but treatments that targeted PD-1/PD-L1 or CTLA-4 showed limited clinical efficacy and did not meet primary endpoints for overall survival5,6. Targeted Therapies Genomic studies of sarcomas have been critical to identifying mutations associated with tumor growth, angiogenesis, and metastasis. These findings led to clinical trials examining the efficacy of tyrosine kinase inhibitors or inhibitors that target vascular endothelial growth factor or insulin-like growth factor-1, but most of these trials failed to meet overall survival endpoints7,8. More recent genomic studies have indicated that mutations associated with different tumors occur in the same genes as some of the targeted therapies, but the mutations differ sufficiently to render these therapies ineffective9. Cellular Immunotherapy Cell-based immunotherapies have shown great promise in treating hematologic malignancies and are being explored for solid tumors. Chimeric antigen receptor (CAR) T cells have been of particular interest as they are patient-derived T cells engineered to express a tumor-specific receptor and thus can target tumors without being detected as foreign cells. Preclinical studies suggested that sarcoma-specific CAR T cells may be effective, but clinical trials have failed due to poor penetration and function of CAR T cells in the immunosuppressive TME10. Recent and ongoing studies are exploring the effects of multi-CAR T cell strategies that target different tumor antigens, as well as the effects of using modified dendritic cells or natural killer cells or combining treatment modalities11. Effective and lasting treatment options for sarcomas continue to be elusive but advances in genomic analysis and immune-based treatments are slowly improving outcomes. Like other cancers, clinical studies exploring treatment combinations are also showing promise and may provide critical breakthroughs for some of the most aggressive sarcomas. 1 Doyle LA. Sarcoma classification: an update based on the 2013 World Health Organization Classification of Tumors of Soft Tissue and Bone. Cancer. 2014 Jun 15;120(12):1763-74. 2 Stahl D, Gentles AJ, Thiele R, Gütgemann I. Prognostic profiling of the immune cell microenvironment in Ewing’s Sarcoma Family of Tumors. Oncoimmunology. 2019 Dec 2;8(12):e1674113. 3 Xiao W, Klement JD, Lu C, Ibrahim ML, Liu K. IFNAR1 controls autocrine type I IFN regulation of PD-L1 expression in myeloid-derived suppressor cells. J. Immunol. 2018 Jul 1;201(1):264-77. 4 Zhu Z, Jin Z, Zhang M, Tang Y, Yang G, Yuan X, Yao J, Sun D. Prognostic value of programmed death-ligand 1 in sarcoma: a meta-analysis. Oncotarget. 2017 Aug 29;8(35):59570. 5 Maki RG, Jungbluth AA, Gnjatic S, Schwartz GK, D’Adamo DR, Keohan ML, Wagner MJ, Scheu K, Chiu R, Ritter E, Kachel J. A pilot study of anti-CTLA4 antibody ipilimumab in patients with synovial sarcoma. Sarcoma. 2013 Oct;2013. 6 Zuo W and Lingdi Z. Recent advances and application of PD-1 blockade in sarcoma." Oncotargets and Therapy 2019; 12:6887. 7 Ray-Coquard IL, Domont J, Tresch-Bruneel E, Bompas E, Cassier PA, Mir O, Piperno-Neumann S, Italiano A, Chevreau C, Cupissol D, Bertucci F. Paclitaxel given once per week with or without bevacizumab in patients with advanced angiosarcoma: a randomized phase II trial. J. Clin. Oncol. 2015 Sep 1;33(25):2797-802. 8 Tap WD, Demetri G, Barnette P, Desai J, Kavan P, Tozer R, Benedetto PW, Friberg G, Deng H, McCaffery I, Leitch I. Phase II study of Ganitumab, a fully human anti–type-1 insulin-like growth factor receptor antibody, in patients with metastatic ewing family tumors or desmoplastic small round cell tumors. J. Clin. Oncol. 2012 May 20;30(15):1849-56. 9 Trédan O, Wang Q, Pissaloux D, Cassier P, de la Fouchardière A, Fayette J, Desseigne F, Ray-Coquard I, de la Fouchardière C, Frappaz D, Heudel PE. Molecular screening program to select molecular-based recommended therapies for metastatic cancer patients: analysis from the ProfiLER trial. Ann. Oncol. 2019 May 1;30(5):757-65. 10 Thanindratarn P, Dean DC, Nelson SD, Hornicek FJ, Duan Z. Chimeric antigen receptor T (CAR-T) cell immunotherapy for sarcomas: From mechanisms to potential clinical applications. Cancer Treatment Reviews. 2020 Jan 1; 82:101934. 11 Patel S, Burga RA, Powell AB, Chorvinsky EA, Hoq N, McCormack SE, Van Pelt SN, Hanley PJ, Cruz CR. Beyond CAR T cells: other cell-based immunotherapeutic strategies against cancer. Front. Onc. 2019 Apr 10; 9:196.

PARP Inhibitors for Ovarian Cancer Treatment
Ovarian cancer remains one of the leading causes of mortality for women with gynecological cancers and continues to be associated with stubbornly low 5-year survival rates. Depending on the stage or type of ovarian cancer, localized treatments including surgical resection or radiation may be sufficient. Treatment of metastatic ovarian cancer may include surgery and radiation combined with chemotherapy. Hormone therapy is also typically combined with chemotherapy for targeted reduction of estrogen and/or stimulation of progesterone for the targeted treatment of ovarian stromal tumors that produce high levels of estrogen. Nonetheless, many of these treatments have limited efficacy for treating metastatic ovarian cancer. Advances in targeted ovarian cancer treatments have been facilitated by identification of cellular replication machinery in some cancer subtypes, including defects in the breast cancer-associated protein (BRCA)1 and BRCA2 genes, which play critical roles in DNA repair and transcription regulation[1]. Poly (ADP-ribose) polymerases (PARP) are a family of enzymes that can repair single strand DNA breaks through the base excision repair pathway[2]. PARPs can work together with normal BRCA1/2 to repair double strand DNA breaks by the homologous recombination (HR) pathway. Preclinical studies have shown that PARP inhibitors are effective in cells with BRCA1/2 mutations because these mutations combined with PARP inhibition cause synthetic lethality due to blockade of multiple DNA repair pathways. Olaparib was the first PARP inhibitor approved for the treatment of germline BRCA1/2-mutated metastatic ovarian cancer in 2014[3]. This treatment was recommended for patients who had undergone three or more rounds of chemotherapy. Olaparib was later approved as a first-line maintenance therapy for germline or somatic BRCA1/2 mutations as well for the treatment of advanced ovarian cancers that have partial or complete responses to first-line platinum-based chemotherapies. Two other PARP inhibitors are also currently approved for different ovarian cancer diagnoses including rucaparib, which is approved for the treatment of germline BRCA1/2 mutations following two rounds of chemotherapy and for maintenance therapy following platinum-based therapies regardless of BRCA mutation status. Similarly, niraparib is approved to treat ovarian cancers with BRCA1/2 mutations or genomic instability and disease progression following platinum-based chemotherapies. Like many other targeted therapies, some patients are completely unresponsive to treatment or develop resistance to PARP inhibitor monotherapy. Recent studies have described promising results associated with combined treatments, including PARP inhibitors combined with anti-angiogenic drugs like bevacizumab[4] or immune check point inhibitors like pembrolizumab[5]. There are currently three ongoing phase III first-line trials comparing the efficacy of combining PARP inhibitors and immune checkpoint blockade with VEGF inhibitors. Several thousand women are being enrolled in these studies with a goal of trying to determine if these combinations improve outcomes[6]. PARP inhibitors continue to be effective for treating hormone receptor-negative tumors but are less effective in treating hormone-receptor-positive ovarian tumors. Current trials are exploring the use of hormone inhibitors to disrupt hormone receptor signaling in ovarian tumors and render them sensitive to PARP inhibition[7]. PARP inhibitors have provided clinical benefits to ovarian cancer patients who previously had limited treatment options. Future studies will likely improve the efficacy of PARP inhibition as a monotherapy or in combination with other targeted therapies. [1] Venkitaraman AR. Functions of BRCA1 and BRCA2 in the biological response to DNA damage. J Cell Sci. 2001 Oct;114(Pt 20):3591-8. [2] D'Amours D, Desnoyers S, D'Silva I, Poirier GG. Poly(ADP-ribosyl)ation reactions in the regulation of nuclear functions. Biochem J. 1999 Sep 1;342 ( Pt 2)(Pt 2):249-68. [3] Franzese E, Centonze S, Diana A, Carlino F, Guerrera LP, Di Napoli M, De Vita F, Pignata S, Ciardiello F, Orditura M. PARP inhibitors in ovarian cancer. Cancer Treatment Reviews. 2019 Feb 1;73:1-9. [4] Ray-Coquard I, Pautier P, Pignata S, Pérol D, González-Martín A, Berger R, Fujiwara K, Vergote I, Colombo N, Mäenpää J, Selle F. Olaparib plus bevacizumab as first-line maintenance in ovarian cancer. New England Journal of Medicine. 2019 Dec 19;381(25):2416-28. [5] Konstantinopoulos PA, Waggoner S, Vidal GA, Mita M, Moroney JW, Holloway R, Van Le L, Sachdev JC, Chapman-Davis E, Colon-Otero G, Penson RT, Matulonis UA, Kim YB, Moore KN, Swisher EM, Färkkilä A, D'Andrea A, Stringer-Reasor E, Wang J, Buerstatte N, Arora S, Graham JR, Bobilev D, Dezube BJ, Munster P. Single-Arm Phases 1 and 2 Trial of Niraparib in Combination with Pembrolizumab in Patients With Recurrent Platinum-Resistant Ovarian Carcinoma. JAMA Oncol. 2019 Aug 1;5(8):1141-1149. [6] Elyashiv, Osnat, Yien Ning Sophia Wong, and Jonathan A. Ledermann. "Frontline Maintenance Treatment for Ovarian Cancer." Current Oncology Reports 23.8 (2021): 1-10.m [7] Matulonis UA, Wulf GM, Barry WT, Birrer M, Westin SN, Farooq S, Bell-McGuinn KM, Obermayer E, Whalen C, Spagnoletti T, Luo W. Phase I dose escalation study of the PI3kinase pathway inhibitor BKM120 and the oral poly (ADP ribose) polymerase (PARP) inhibitor olaparib for the treatment of high-grade serous ovarian and breast cancer. Annals of Oncology. 2017 Mar 1;28(3):512-8.
Current Trends in Gastrointestinal Cancer – CRISPR/Cas9-based Immunotherapy
Gastrointestinal cancers are a heterogeneous group of cancers that can be caused by H. pylori bacterial or Epstein-Barr virus infection, chronic inflammation, or inherited or spontaneous genetic mutations. Advances in solid tumor immunotherapy for gastrointestinal cancers include the development of methods that improve the screening, evaluation, and development of more precise and robust treatments. Breakthroughs in basic and translational research are leading to better treatment options for gastrointestinal cancer, and CRISPR/Cas9-based (clustered regularly interspaced short palindromic repeats/CRISPR-associated protein 9) gene editing technology is at the forefront of these discoveries. CRISPR/Cas9-based gene editing technology was originally identified in bacteria and archaea as an antiviral defense mechanism[1]. As a gene editing application, CRISPR/Cas9 uses the Cas9 nuclease to cleave specific sequences in the target DNA and introduces modifications such as knock-in or knock-out mutations[2]. The DNA sequence is targeted using a single-guide RNA (sgRNA) comprised of CRISPR RNA (crRNA) and trans-activating CRISPR RNA (tracRNA), and these RNAs can be expressed on the same plasmid as the Cas9 nuclease upon delivery into target cells. The crRNA/tracrRNA duplex can bind to the complementary sequence in the genomic DNA and recruit Cas9, which cleaves the target sequence and allows for DNA repair by either homology-directed repair or non-homologous end pairing. This repaired sequence is now a part of the genomic DNA and leaves virtually no trace of gene editing. CRISPR/Cas9 gene editing has been used for several applications in oncology research and more recently to improve immune-oncology strategies. One of the earliest applications involves knockout screens in which a library of sgRNAs is used to transfect a pool of knockouts that can be used for gain-of-function or small molecule/drug screens. Genome-wide screens of cancer cell lines have been useful in identifying genes that are essential to cancer cell growth but can be prone to false-positive hits if the screens are not correctly designed or analyzed[3]. Genome-wide screens have also been used to identify genes linked to resistance, and such gene hits have been identified in a melanoma library screen when treating with the inhibitor vemurafenib[4]. Combinatorial CRISPR/Cas9 screens are now being used to target multiple genes, and this approach can be used for defining genetic or cellular pathways involved in cancer or characterizing drugs that target multiple genes[5]. CRISPR/Cas9 has moved beyond in vitro cell culture and can be used for human organoid models for studying oncogenesis. ARID1A is one of the most frequently mutated genes in solid tumors, including gastric tumors[6]. ARID1A encodes a BAF complex subunit that normally targets BAF to AT-rich DNA sequences to regulate transcription. Mouse studies have suggested that ARID1A is involved in gastrointestinal cancer oncogenesis, but this was not validated in humans until a recent study that used CRISPR/Cas9-mediated depletion of ARID1A wild-type human gastric organoids. This ARID1A-knockout organoid system established a forward genetics model of gastric cancer that resembled gastric cancer phenotypically and identified BIRC5/Survivin as a key player in early tumorigenesis. This type of organoid model is not only useful for basic oncogenesis studies but can be used for small molecule inhibitor screens. CRISPR/Cas9 screens can be used to validate mutations found in patients with gastrointestinal tumors. Activin A receptor type 2A (ACVR2A) is frequently mutated in patients with microsatellite instability-high gastric cancer, and a 2021 study used CRISPR/Cas9 to generate ACVR2A-knockout human gastric cancer cells[7]. These cells exhibited less aggressive proliferation, migration, and invasion in vitro, and patients with ACVR2A mutations had better prognoses than patients with wild-type ACVR2A. Gastrointestinal stromal tumors (GIST) have been typically characterized by activation mutations in the receptor tyrosine kinase KIT, but a 2022 study using genome-wide CRISPR screening identified the complementary chromatin-modifying complexes MOZ and Menin-MLL as being essential to GIST[8]. This finding highlights a trend in oncology research elucidating a role for chromatin regulation in tumorigenesis, which has the potential to be targeted therapeutically. Beyond basic research, CRISPR/Cas9 is starting to be used in applications for clinical trials. A Phase II trial has recently launched that is using CRISPR/Cas9 to delete an intracellular checkpoint molecule called cytokine-induced SH2 (CISH) protein[9]. Preclinical studies have shown that CRISPR/Cas9-mediated deletion of CISH enhanced antitumor responses, and the Phase II trial is using patient-derived CRISPR-modified T cells to treat individuals with metastatic gastrointestinal tumors. CAR T-cells (Chimeric Antigen Receptor) have been an incredible progress in personalized therapy targeting cancer.[10] However, different challenges hampered the availability, efficacy, and safety of this promising cell therapy. CRISPR-Cas9 technology can address many of these limitations. Desired genetic modification can be achieved with cellular precision engineering, leveraging CRISPR-Cas9-based gene editing. In addition, this approach can be exploited to overcome T-cell exhaustion, lack of CAR T-cell persistence, and toxicity related to cytokine release. In particular, the implementation of CRISPR-Cas9 technology generated universal CAR T Cells resistant to PD1 Inhibition; or enhanced T cell function against bladder cancer disrupting CTLA-4.[11] In the oncolytic therapy field, it has been demonstrated that HSV-1-derived CD40L-armed oncolytic therapy by CRISPR-Cas9-based gene editing boosted endogenous immunity in pancreatic ductal adenocarcinoma.[12] CRISPR/Cas9 gene editing will continue to transform basic and clinical research, immunotherapy, and cellular therapy providing effective and safe therapeutic strategies. Regulatory agencies are now developing frameworks to allow for the use of this revolutionary tool in a wide range of diseases. [1] Wiedenheft B, Sternberg SH, Doudna JA. RNA-guided genetic silencing systems in bacteria and archaea. Nature. 2012 Feb 15;482(7385):331-8. [2] Barrangou R, Doudna JA. Applications of CRISPR technologies in research and beyond. Nat. Biotechnol. 2016;34(9):933-941. [3] Munoz DM, Cassiani PJ, Li L, Billy E, Korn JM, Jones MD, Golji J, Ruddy DA, Yu K, McAllister G, DeWeck A. CRISPR screens provide a comprehensive assessment of cancer vulnerabilities but generate false-positive hits for highly amplified genomic regions. Cancer Discovery. 2016 Aug 1;6(8):900-13. [4] Shalem O, Sanjana NE, Hartenian E, Shi X , Scott DA , et al. Genome-scale CRISPR-Cas9 knockout screening in human cells. Science. 2014. 343:84–87. [5] Han K, Jeng EE, Hess GT, Morgens DW, Li A, Bassik MC. Synergistic drug combinations for cancer identified in a CRISPR screen for pairwise genetic interactions. Nat. Biotechnol. 2017 May;35(5):463-74. [6] Lo YH, Kolahi KS, Du Y, Chang CY, Krokhotin A, Nair A, Sobba WD, Karlsson K, Jones SJ, Longacre TA, Mah AT, Tercan B, Sockell A, Xu H, Seoane JA, Chen J, Shmulevich I, Weissman JS, Curtis C, Califano A, Fu H, Crabtree GR, Kuo CJ. A CRISPR/Cas9-Engineered ARID1A-Deficient Human Gastric Cancer Organoid Model Reveals Essential and Nonessential Modes of Oncogenic Transformation. Cancer Discov. 2021 Jun;11(6):1562-1581. [7] Yuza K, Nagahashi M, Ichikawa H, Hanyu T, Nakajima M, Shimada Y, Ishikawa T, Sakata J, Takeuchi S, Okuda S, Matsuda Y, Abe M, Sakimura K, Takabe K, Wakai T. Activin a Receptor Type 2A Mutation Affects the Tumor Biology of Microsatellite Instability-High Gastric Cancer. J. Gastrointest. Surg. 2021 Jan 8. doi: 10.1007/s11605-020-04889-9. Epub ahead of print. [8] Hemming ML, Benson MR, Loycano MA, Anderson JA, Andersen JL, Taddei ML, Krivtsov AV, Aubrey BJ, Cutler JA, Hatton C, Sicinska E. MOZ and Menin-MLL Complexes are Complementary Regulators of Chromatin Association and Transcriptional Output in Gastrointestinal Stromal Tumor. Cancer Discovery. 2022 May 2. [9] https://twin-cities.umn.edu/news-events/university-minnesota-opens-first-its-kind-clinical-trial-treat-metastatic-gi-cancers [10] Jogalekar MP, Rajendran RL, Khan F, Dmello C, Gangadaran P, Ahn BC.Front Immunol. 2022 Jul 22;13:925985. doi: 10.3389/fimmu.2022.925985. eCollection 2022. [11] Zhang W, Shi L, Zhao Z, Du P, Ye X, Li D, Cai Z, Han J, Cai J. Disruption of CTLA-4 expression on peripheral blood CD8 + T cell enhances anti-tumor efficacy in bladder cancer. Cancer Chemother Pharmacol. 2019;83:911–20. [12] Wang R, Chen J, Wang W, Zhao Z, Wang H, Liu S, et al. CD40L-armed oncolytic herpes simplex virus suppresses pancreatic ductal adenocarcinoma by facilitating the tumor microenvironment favorable to cytotoxic T cell response in the syngeneic mouse model. J Immunother Cancer. 2022;10(1):e003809.

Insights in Invasive Bladder Cancer
Bladder cancer is a relatively common form of cancer that is defined as either pre-invasive or invasive, and non-muscle invasive bladder cancer (NMIBC) is the most commonly diagnosed subtype[1]. NMIBC is typically treated by surgical resection and/or intravesical delivery of chemo- or immunotherapy-based adjuvant treatment, and long-term efficacy is monitored by urine testing or cystoscopy. Muscle-invasive bladder cancer (MIBC) is relatively resistant to current treatment options and occurs more frequently in men. MIBC also has high rates of morbidity and mortality, and novel therapies or combination therapies are being developed to better treat this form of bladder cancer. Here we highlight recent findings about invasive bladder cancer biology and how these observations are informing the development of new therapies. Mutation Landscape Analysis of MIBC genomes has revealed a high mutation rate in tumors that approaches rates seen in melanoma and lung cancer[2]. The mutational signature of many MIBC tumors is consistent with mutations associated with APOBEC (apolipoprotein B mRNA-editing enzyme, catalytic polypeptide-like) cytidine deaminase, and many of the mutations are clonal, which suggests that the effects of APOBEC expression in bladder tissue occurs early in tumorigenesis. Non-invasive and invasive bladder tumors are also often classified as being highly heterogeneous, and tumor histology can be extremely variable and includes squamous, plasmacytoid, micropapillary, and small-cell carcinoma. This molecular and histological heterogeneity presents a challenge in subtyping tumors based on gene expression profiles and provides insight into why it can be difficult to identify targeted therapies that are effective against bladder cancers. Several genes are commonly mutated in both NMIBC and MIBC, but mutation rates for some of these genes, including MLL2 and TP53, are higher in invasive tumors[3]. TP53 mutations appear to be a critical factor associated with the transition to its invasive form. Mutations have also been identified in genes associated with the sister chromatid cohesion and segregation process (STAG2, ESPL1, FGFR3, and TACC3)[3] and chromatin remodeling (UTX, MLL-MLL3, CREBBP-EP300, NCOR1, ARID1A, and CHD6)[4]. Immunotherapy Insights NIMBC is one of the first forms of cancer treated with an immunotherapy approach in which the attenuated tuberculosis bacterial vaccine, Bacillus Calmette-Guérin (BCG), is delivered intravesically to the bladder and triggers an immune response that inhibits tumor growth[5]. Recently, immune checkpoint inhibitor-based treatments have been examined as therapeutic options for different bladder cancers. Expression of the PD-L1 immune checkpoint molecule has been detected on both NIMBC and MIBC tumor cells and tumor-infiltrating mononuclear cells. Antibody-based blockade of PD-1/PD-L1 interactions restores anti-tumor responses mediated by T cells. Atezolizumab was the first PD-L1 inhibitor approved for the treatment of locally advanced/ metastatic urothelial carcinoma (LA/mUC) that has progressed or after cisplatin-based chemotherapy[6], and five different PD-L1/PD-1 inhibitors have been approved for this form of bladder cancer. Other checkpoint inhibitors that target different molecules have not shown significant improvements in overall survival or progression-free survival. Clinical trials currently underway are examining the efficacy of combinations of checkpoint inhibitors or the use of these inhibitors as an adjuvant therapy to surgical resection or chemotherapy. In addition, therapies that target specific mutations, such as FGFR, HER2, or chromatin-modifying genes, are also under investigation, and the FGFR inhibitor erdafitinib was recently approved for the treatment of LA/mUC[7][8]. Bladder cancer treatment outcomes continue to advance because of insights into the basic biology of bladder cancer, and a better understanding of molecular and immunological mechanisms associated with anti-tumor responses. The many preclinical and clinical studies currently underway for bladder cancer will contribute valuable information to new therapeutic options, especially for patients with refractory or invasive forms of bladder cancer. [1] Knowles MA, Hurst CD. Molecular Biology of Bladder Cancer: New Insights into Pathogenesis and Clinical Diversity. Nat Rev Cancer. 2015;15:25–41. [2] Robertson AG, Kim J, Al-Ahmadie H, et al. Comprehensive Molecular Characterization of Muscle-Invasive Bladder Cancer. Cell. 2017;171(3):540-556.e25. [3] Guo G, Sun X, Chen C, et al. Whole-Genome and Whole-Exome Sequencing of Bladder Cancer Identifies Frequent Alterations in Genes Involved in Sister Chromatid Cohesion and Segregation. Nat Genet. 2013;45(12):1459-1463. [4] Gui Y, Guo G, Huang Y, et al. Frequent Mutations of Chromatin Remodeling Genes in Transitional Cell Carcinoma of the Bladder. Nat Genet. 2011;43(9):875-878. [5] Herr HW and Morales A. History of Bacillus Calmette-Guerin and Bladder Cancer: An Immunotherapy Success Story. J Urol. 2008;179.1: 53-56. [6] Bellmunt J, Powles T, Vogelzang NJ. A Review on the Evolution of PD-1/PD-L1 Immunotherapy for Bladder Cancer: The Future is Now. Cancer Treat. Rev. 2017;54:58-67. [7] Osterman CK, Milowsky MI. New and Emerging Therapies in the Management of Bladder Cancer. F1000Res. 2020;9:F1000 Faculty Rev-1146. 1 [8] Loriot Y, Necchi A, Park SH, et al. Erdafitinib in Locally Advanced or Metastatic Urothelial Carcinoma. N Engl J Med. 2019 Jul 25;381(4):338-348.

Head & Neck Cancers - New Mutation Insights Lead to New Therapies
Head and neck squamous cell carcinoma (HNSCC) is one of the most common forms of cancer in the world. This heterogeneous disease is most often seen in men and is closely linked to tobacco usage, which can be enhanced by alcohol usage. Human papillomavirus (HPV) infection is an independent risk factor for HNSCC[1], and most HPV- HNSCCs occur in the larynx and oral cavity, and HPV+ HNSCCs typically arise in the oropharynx[2]. Both HPV+ and HPV- HNSCCs are typically diagnosed at advanced disease stages and are often treated with an aggressive combination of surgery, radiotherapy (RT), and chemotherapy[3]. More recently, cetuximab, an IgG1 monoclonal antibody that targets epidermal growth factor receptor (EGFR) has been used in combination with radiotherapy and has shown some improvements in progression-free survival (PFS) and overall survival (OS)[4]. Advances in genomic technology have provided critical insights into the pathology of HNSCC subtypes. Some HNSCCs are now known to have high mutational burdens, which is like other cancers associated with carcinogen exposure. Analysis of HPV- and HPV+ HNSCCs in The Cancer Genome Atlas (TGCA) network has been instrumental in identifying genome defects common to both HPV+ and HPV- HNSCCs, as well as defects that are unique to each of these subtypes. Global analysis of all HNSCC subtypes identified TP53 as the most commonly mutated gene, but there tends to be a lower percentage of TP53 mutations in HPV+ tumors versus HPV- tumors, likely related to HPV infection[5]. Activating mutations in PIK3CA and inactivating mutations in NOTCH1 are associated with both types of HNSCC. HPV- HNSCCs show inactivating mutations in TP53 and CDKN2A cell cycle suppressor genes and amplification of CCND1, which can all contribute to unchecked cell cycle progression. In contrast, HPV+ HNSCCs show expression of the E6 and E7 viral oncogenes, which can inhibit TP53 and RB1, as well as activation of cell cycle regulator E2F1[6]. Mutations in the MAPK signaling component HRAS have also been identified in a fraction of HNSCC specimens for which treatment options are limited. A recent clinical trial demonstrated encouraging efficacy in patients with recurring or metastatic HNSCCs carrying HRAS mutations[7] treated with tipifarnib, which is a farnesyltransferase inhibitor that can inhibit farnesylation of HRAS and membrane targeting and downstream signaling. In addition to targeted therapies, recent studies suggest that PD-1/PD-L1 blockade alone or in combination with chemotherapy can improve overall survival in patients with recurrent or metastatic HNSCC[8],[9]. PD-1 blockade has shown better survival, toxicity, and response duration compared with cetuximab treatment combined with chemotherapy, but these responses are dependent on patients having HNSCC tumors that are positive for PD-L1. Tumor mutational burden and the expression of inflammatory biomarkers also correlated directly with responses to PD-1 blockade. Recent insights into genomic variations associated with HNSCC subtypes are providing valuable information with respect to basic tumor biology as well as identifying potential therapeutic targets for preclinical development. [1] Cognetti DM, Weber RS, Lai SY. Head and neck cancer: an evolving treatment paradigm. Cancer. 113(7 Suppl):1911-1932 (2008). [2] Mehanna H, Beech T, Nicholson T, El-Hariry I, McConkey C, Paleri V, Roberts S. Prevalence of human papillomavirus in oropharyngeal and nonoropharyngeal head and neck cancer--systematic review and meta-analysis of trends by time and region. Head Neck. 35(5):747–55 (2013). [3] Pignon J P, le Maître A, Maillard E, Bourhis J. & MACH-NC Collaborative Group. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomized trials and 17,346 patients. Radiother. Oncol. 92(1), 4–14 (2009). [4] Bonner JA, et al. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomized trial, and the relation between cetuximab-induced rash and survival. Lancet Oncol. 11, 21–28 (2010). 5] Westra, W. H. et al. The inverse relationship between human papillomavirus-16 infection and disruptive p53 gene mutations in squamous cell carcinoma of the head and neck. Clin. Cancer Res. 14, 366–369 (2008) [6] Beck TN, Golemis EA. Genomic insights into head and neck cancer. Cancers Head Neck 1, 1 (2016). [7] Ho AL, Brana I, Haddad R. et al. Tipifarnib in Head and Neck Squamous Cell Carcinoma with HRAS Mutations. J. Clin. Oncol. JCO2002903 (2021). [8] de Sousa LG, Ferrarotto R. Pembrolizumab in the first-line treatment of advanced head and neck cancer. Expt. Rev. Anticanc. Ther. 21.12: 1321-1331 (2021). [9] Haddad RI, Seiwert TY, Chow LQM et al. Influence of tumor mutational burden, inflammatory gene expression profile, and PD-L1 expression on response to pembrolizumab in head and neck squamous cell carcinoma. J. Immunother. Cancer. 2022 Feb;10(2):e003026.
Targeted Therapy for Biliary Cancers
Biliary tract cancers, which are also known as cholangiocarcinomas (CCA), describe malignancies that occur in the biliary tract and include the pancreas, gallbladder, and bile ducts. These are relatively rare cancers but are associated with a poor prognosis given that these cancers are difficult to detect and are usually diagnosed at later stages of the disease. Current CCA classification and clinical care CCAs are classified by growth pattern as mass forming, intraductal, or periductal, anatomical location as intrahepatic or extrahepatic (perihilar, or distal), and histology (predominantly adenocarcinomas with mixed hepatocellular CCAs are defined as a separate subtype of primary hepatic cancer) [1]. CCAs can arise de novo with no discernable risk factors, but a variety of genetic and nongenetic risk factors are associated with CCA, including liver cirrhosis, obesity, type 2 diabetes, chronic hepatitis B or C infection, or infection with hepatobiliary flukes [2]. Individuals with primary sclerosing cholangitis have higher levels of chronic liver inflammation and increased incidence of CCA [3] as well. CCAs are typically aggressive cancers with a median overall survival of < 24 months. The only treatment options have been surgical resection or liver transplantation for early-stage patients or aggressive chemotherapy for patients with advanced stages of the disease [4]. CCA molecular classification Next-generation sequencing technology has allowed the identification of molecular subtypes associated with several gene mutations that are linked to increased CCA risk, including mutations in chromatin remodeling genes (ARID1A, BAP1, and PBRM1) [5,6]. IDH1 mutations have been linked to intrahepatic CCA and mutations in ERBB2 are more closely associated with extrahepatic CCA [7]. Mutations in the fibroblast growth factor (FGF) signaling pathway, including mutations or translocations in FGF receptor (FGFR) genes, have also been identified in CCA, and an FGFR fusion has been linked specifically to intrahepatic CCA [8]. Moreover, patients with IDH1/2 mutations also exhibit elevated FGFR expression, even without FGFR mutations or fusions, further affirming a role for FGF/FGFR signaling in CCA progression[9]. In addition to tumor cell alterations, the tumor microenvironment is also being extensively explored and has led to the identification of an inflamed intrahepatic CCA subtype potentially treatable with checkpoint blockade immunotherapy [10]. New CCA precision therapies The FGF/FGFR pathway has become one of the most encouraging targets for novel CCA therapeutics. As FGFRs are receptor tyrosine kinases, nonselective FGFR inhibitors that target the conserved ATP-binding domain were the first drugs to be tested in clinical trials. A recent trial exploring the use of the nonselective FGFR kinase inhibitor pazopanib combined with a MEK inhibitor showed little efficacy [11]. Pemagatinib is the first FDA-approved targeted therapy for advanced CCA with FGFR2 fusions or rearrangements. Pemagatinib is a selective inhibitor of FGFR1, 2, and 3 and was approved in 2020 and given breakthrough therapy designation as the first drug to specifically treat CCA [12]. In 2021, Ivosidenib (Tibsovo), a small molecule IDH1 inhibitor, was approved by the FDA for treating IDH1 mutated locally advanced or metastatic CCA [13]. Very recently, the FDA has granted accelerated approval to two FGFR inhibitors: Infigratinib (Truseltiq), for the treatment of previously treated, unresectable, locally advanced or metastatic cholangiocarcinoma with FGFR2 fusion (and a companion diagnostic to identify patients eligible to receive this treatment) [14,15]; and Futinatinib (TAS-120) for patients with previously treated, unresectable, locally advanced or metastatic intrahepatic CCA with FGFR2 gene fusions or other rearrangements [16,17]. Alternative FGF/FGFR inhibitors are also under development and target the extracellular domain or function as FGF ligand traps [18]. These alternative inhibitors can be used potentially in combination with FGFR kinase inhibitors that have lost efficacy due to the development of resistance [19]. In addition to mutation-driven therapeutic approaches, immune checkpoint inhibitors are currently tested in combination with chemotherapy to improve efficacy. A very recent study conducted on patients with advanced biliary tract cancer showed that Durvalumab, a PD-L1 inhibitor, significantly improves survival compared to chemotherapy alone [20]. New research on novel inhibitors and combination therapies will likely identify other therapeutic options for CCA, and these cancers will not be the terminal diagnoses they once were. Razumilava N, Gores Cholangiocarcinoma. Lancet. 2014;383(9935):2168- 79. Yao KJ, Jabbour S, et al. Increasing mortality in the United States from cholangiocarcinoma: an analysis of the National Center for Health Statistics Database. BMC Gastroenterol. 2016;16(1):117. Hirschfield GM, Karlsen TH, et Primary sclerosing cholangitis. Lancet. 2013;382(9904):1587-99. Yazici C, Niemeyer DJ, et al. Hepatocellular carcinoma and cholangiocarcinoma: an Expert Rev Gastroenterol Hepatol. 2014;8(1):63-82. Jusakul A, Cutcutache I, et al. Whole‐genome and epigenomic landscapes of etiologically distinct subtypes of cholangiocarcinoma. Cancer Discov 2017;7:1116‐1135 Jiao Y, Pawlik TM, et al. Exome sequencing identifies frequent inactivating mutations in BAP1, ARID1A, and PBRM1 in intrahepatic Nat Genet. 2013;45:1470–3. Churi CR, Shroff R, et Mutation profiling in cholangiocarcinoma: prognostic and therapeutic implications. PLoS One. 2014;9:e115383. Graham RP, Barr Fritcher EG, et al. Fibroblast growth factor receptor 2 translocations in intrahepatic Hum Pathol. 2014;45(8):1630- 1638. Wang P, Dong Q, et Mutations in isocitrate dehydrogenase 1 and 2 occur frequently in intrahepatic cholangiocarcinomas and share hypermethylation targets with glioblastomas. Oncogene. 2013;32(25):3091-3100. Job S, Rapoud D, et al.. Identification of Four Immune Subtypes Characterized by Distinct Composition and Functions of Tumor Microenvironment in Intrahepatic Cholangiocarcinoma. Hepatology. 2020 Sep;72(3):965-981 Shroff RT, Yarchoan M, O’Connor A, et The oral VEGF receptor tyrosine kinase inhibitor pazopanib in combination with the MEK inhibitor trametinib in advanced cholangiocarcinoma. Br J Cancer. 2017;116(11):1402-1407. Patel TH, Marcus L, et al. FDA Approval Summary: Pemigatinib for Previously Treated, Unresectable Locally Advanced or Metastatic Cholangiocarcinoma with FGFR2 fusion or other rearrangements. Clin Cancer Res. 2022 Oct 7:CCR-22-2036. Sumbly V, Landry I, Rizzo V. Ivosidenib for IDH1 Mutant Cholangiocarcinoma: A Narrative Review. Cureus. 2022 Jan 7;14(1):e21018 Javle M, Roychowdhury S, et al. Infigratinib (BGJ398) in previously treated patients with advanced or metastatic cholangiocarcinoma with FGFR2 fusions or rearrangements: mature results from a multicentre, open-label, single-arm, phase 2 study. Lancet Gastroenterol Hepatol. 2021 Oct;6(10):803-815. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-infigratinib-metastatic-cholangiocarcinoma Goyal L, Meric-Bernstam F, et al. Futibatinib for FGFR2-Rearranged Intrahepatic Cholangiocarcinoma. N Engl J Med. 2023 Jan 19;388(3):228-239. doi: 10.1056/NEJMoa2206834. PMID: 36652354. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-futibatinib-cholangiocarcinoma Tolcher AW, Papadopoulos KP, Patnaik A, et A phase I, first in human study of FP-1039 (GSK3052230), a novel FGF ligand trap, in patients with advanced solid tumors. Ann Oncol. 2016;27(3):526-532. Touat M, Ileana E, et Targeting FGFR signaling in cancer. Clin Cancer Res. 2015;21(12):2684-2694. https://meetings.asco.org/abstracts-presentations/204876
Evaluating DNA Damage in Preclinical PDX Models
DNA damage is one of the primary triggers of cancer development and has been linked to many types of cancers, including prostate, stomach, liver, and skin cancers, as well as leukemia. Within cells, the DNA sequence encodes all the instructions required for building proteins that are needed for cellular functions such as metabolism, replication, tissue, and organ maintenance. The fidelity of the DNA sequence in a cell is maintained by multiple mechanisms, including the DNA damage repair mechanism, but errors and mutations can occur, which sets off a chain of events that leads to tumor growth. DNA damage can be caused by exogenous sources, such as UV radiation, chemical carcinogens, and infection with human papillomavirus or Helicobacter pylori. Endogenous DNA damage can also be caused by multiple factors, including unchecked metabolites like reactive oxygen species (ROS) and defects in DNA damage repair enzymes. Since DNA damage mechanisms have been known to cause numerous cancers, several drugs, particularly small molecule inhibitors, have been developed to target DNA damage repair pathways. Improvements in animal models for cancer have revolutionized how anti-cancer drugs are evaluated and developed, including drugs targeting DNA damage. Patient-derived xenograft (PDX) models have been particularly powerful tools since they use patient-derived tumor tissue engrafted into mice. Tumor cell lines, solid tumor tissue, or hematological tumors can be transplanted into immunodeficient mice to study DNA damage repair mechanisms. These immunocompromised mice can also be humanized by inoculating human immune cells or made to express components of the human immune system, like immune checkpoint molecules, to better screen for the effectiveness of various anti-cancer treatments. In this era of rapid, high-throughput DNA sequencing, individual tumors can be sequenced and specific defects in DNA damage repair pathways can be defined. This same tumor tissue can be engrafted into a PDX mouse model for screening of drugs or therapeutics that tackle the appropriate DNA damage repair defect. Different assays can also be used to study DNA damage and repair mechanisms: comet assay is used to detect DNA single/double-strand breaks in single cells, γH2AX detection by IHC staining or western blot can be used to detect, measure, and localize DNA breaks. This approach is powerful for screening preclinical drug candidates targeting DNA damage and repair for efficacy against a range of tumors and it also provides insights into potential off-target effects or toxicities. From the patient's perspective, pre-screening potential treatment options in mice can lead to the selection of the most appropriate drug or therapeutic targeting DNA damage and repair and help avoid treatments that may be ineffective. DNA damage events can lead to tumor growth and this area of research continues to inform drug development on the bench and patient care in the clinic. Champions Oncology is the ideal partner to accelerate your DNA damage-targeted drug pipeline. We offer a large bank of PDX models, particularly PDX models with high microsatellite instability (MSI-H), that have dysregulated DNA damage repair mechanisms, for ex vivo and in vivo studies. We also provide DNA sequencing, comet assay, and γH2AX detection by IHC staining or western blot, to support your DNA damage targeting drug programs. To add DNA damage evaluation to your upcoming study, contact us today.