In our last blog post, we explored why resistance has become the defining challenge in KRAS drug development.
As the field has matured, it has become clear that early activity alone is not enough, and understanding why tumors respond or not, and how they escape treatment is now essential. It also raises the deeper issue of if response and resistance vary so widely, then a critical assumption at the heart of many programs needs to be challenged:
Can “KRAS-mutant” still be treated as a single category in drug development?
The evidence increasingly suggests the answer is no.
The problem with treating KRAS as one market
As KRAS-targeted therapies have moved forward, many development strategies have been framed broadly around “KRAS-mutant tumors.” On the surface, this makes sense as KRAS is one of the most common oncogenic drivers across multiple cancer types. However, in practice, this simplification hides important biological differences.
Across KRAS-mutant tumors, responses to targeted therapies are highly variable, with some settings showing meaningful activity, while others demonstrating limited or short-lived responses. Even within the same tumor type, outcomes can differ significantly across patients. This variability is not random and reflects the underlying biological context, which now matters more than ever.
Allele matters more than ever
Not all KRAS mutations are the same, with variants such as G12C, G12D, and G12V differing in their biochemical properties, downstream signaling behavior, and sensitivity to targeted inhibition. As more therapies are developed beyond the initial wave of KRAS G12C inhibitors, these differences are becoming increasingly relevant.
Emerging preclinical data shows that response patterns can vary across KRAS allele types, influencing both the depth and durability of response.
For drug developers, this means that evaluating an asset against a generic “KRAS-mutant” panel is no longer sufficient, and the real question to now ask is: Which KRAS variants does your therapy work against, and under what conditions?
Co-mutations shape response and resistance
KRAS does not operate in isolation. Tumors often carry additional genetic alterations that influence pathway signaling, tumor behavior, and therapeutic response. These co-driver mutations can enhance sensitivity in some contexts or drive resistance in others.
Across clinically relevant models, differences in co-mutation profiles have been linked to distinct response patterns and resistance mechanisms, which has two important implications:
- A therapy that appears broadly effective in a simplified model system may fail in more complex, clinically representative settings.
- Co-mutation context can represent an opportunity. Understanding these relationships can help identify patient subsets that are more likely to benefit or reveal combination strategies that overcome resistance.
Tumor type defines the biological landscape
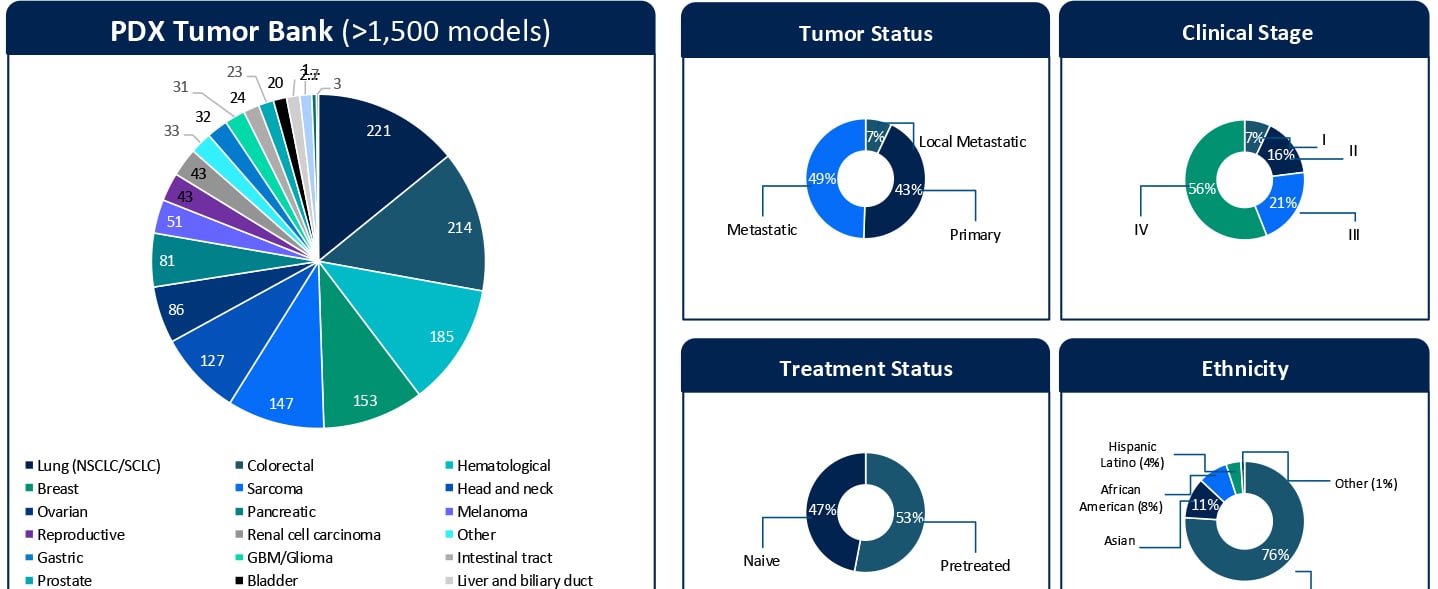
KRAS mutations occur across multiple tumor types, including non-small cell lung cancer, colorectal cancer, and pancreatic ductal adenocarcinoma. Each tumor type exists within its own biological environment, shaped by factors such as tissue origin, microenvironment, and lineage-specific signaling networks. These differences influence how KRAS-driven pathways behave and how tumors respond to targeted therapies.
As a result, a therapy that performs well in one indication may not translate directly to another. This is why preclinical strategies must be designed with indication in mind. Testing a KRAS program in the wrong context can lead to misleading conclusions about its potential.
Why context-aware model selection is critical
Taken together, these factors make one thing clear: Context is a requirement, rather than a refinement.
Effective KRAS studies must move beyond generic model selection and instead reflect the biological diversity seen in the clinic, which includes:
- Selecting models that represent specific KRAS variants
- Capturing diverse co-mutation landscapes
- Matching studies to relevant tumor types
- Incorporating clinically meaningful patient characteristics
Modern preclinical platforms are increasingly designed to meet these needs by combining deeply characterized patient-derived models with molecular and clinical annotation.
This approach allows teams to design studies that are not only more realistic, but also more informative.
Better context leads to better decisions
When KRAS programs are evaluated within the right biological context, the quality of decision-making improves significantly, allowing teams to:
- Rank assets more accurately
- Identify the most promising indications
- Develop more precise biomarker strategies
- Design more rational clinical trials
Perhaps, most importantly, they can avoid overinterpreting results that may not translate outside of a narrow experimental setting.
In a competitive and rapidly evolving field, this clarity can make the difference between advancing the right candidate and pursuing a path that ultimately fails in the clinic.
From resistance to real-world biology
In our previous article, we highlighted the importance of modeling resistance to understand how tumors respond over time, and in this post we have expanded on that idea.
Resistance does not emerge in a vacuum. It is shaped by the biological context of the tumor, including allele, co-mutation, and tumor type. Ignoring that context risks misunderstanding both response and resistance.
What comes next
If biological context shapes response, then treatment history is another critical factor that must be considered. In reality, most patients entering clinical trials are not treatment-naive. Their tumors have been shaped by prior therapies, and those therapies influence how they respond to potential new agents.
In our next post in this series, we will explore why treatment-naive models are increasingly insufficient and why pretreated, clinically aligned models are essential for studying KRAS programs in today’s landscape.
Talk to us
If you are developing a KRAS-targeted therapy, understanding how allele, co-mutation, and tumor type shape response is no longer optional. Talk to our team about designing context-aware preclinical studies that generate data you can trust and act on.