The Tumor Microenvironment: A Barrier to Effective Cancer Therapy
The tumor microenvironment or TME is critical in shaping tumor progression, therapy resistance, and recurrence. The tumor microenvironment comprises stromal cells, immune cells, and signaling molecules that significantly impact how tumors respond to treatment. Immunosuppressive components of the tumor microenvironment, such as M2-polarized macrophages and activated cancer-associated fibroblasts (CAFs), foster resistance to therapies by creating an environment where immune responses are suppressed, and tumor survival is promoted. Key cytokines like IL-10 and TGF-β drive this immunosuppressive milieu, hindering the efficacy of immunotherapies and other anti-cancer treatments.
Despite advancements, many cancer therapies fail in the clinical setting because the preclinical models used to evaluate them inadequately replicate the human tumor microenvironment. Addressing this issue is crucial for developing treatments that overcome tumor microenvironment-induced resistance and enhance clinical outcomes.
The Limitations of Current Preclinical Models
In Vivo Models: The Gold Standard, But Not Without Flaws
In vivo models, particularly mouse models, have long been considered the gold standard for preclinical cancer research. However, they are not perfect, and it is important to know their limitations to navigate the field and select the right model for every application.
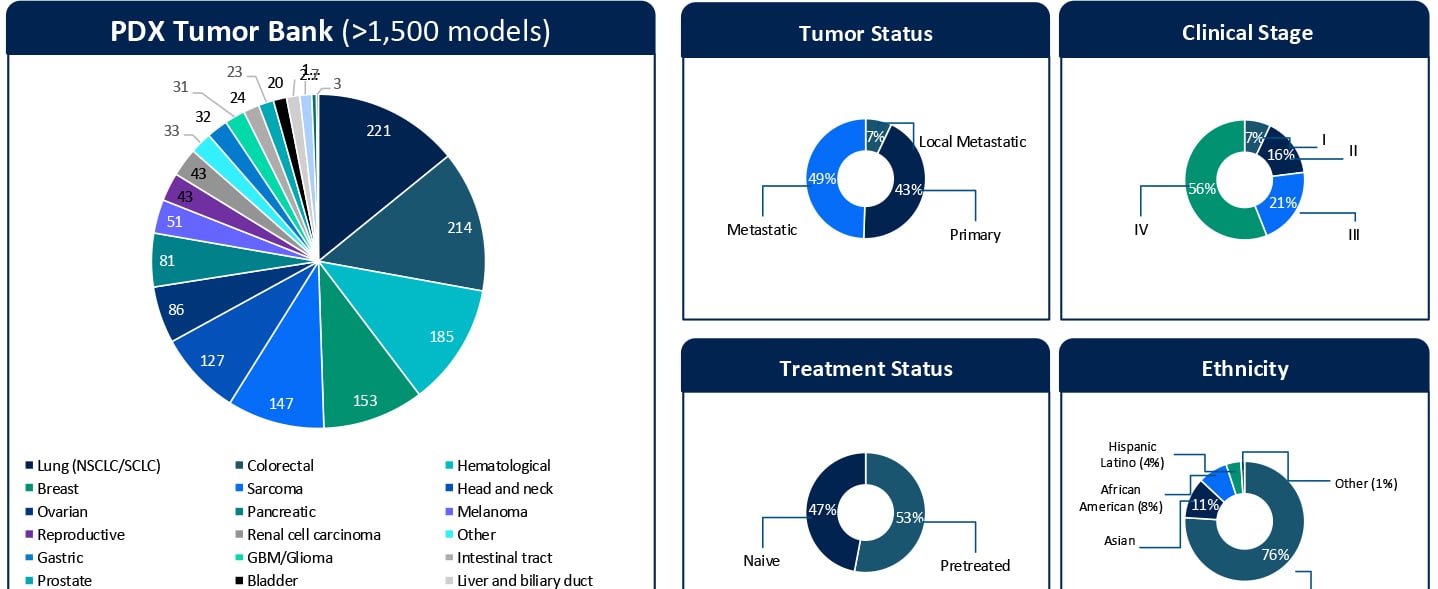
While patient-derived xenografts (PDXs) maintain the genetic and histopathological features of human tumors and are considered an optimal model for clinical translatability of pre-clinical testing, the stromal compartment—including vasculature, immune cells, and fibroblasts—originates from the mouse host. This murine stroma fails to fully replicate the complexity and behavior of the human tumor microenvironment, limiting translational relevance.
Humanized mouse models attempt to overcome some of these limitations by engrafting human immune cells into immunodeficient mice. While this approach provides valuable insights into immuno-oncology, it does not incorporate other critical human stromal components, such as CAFs and endothelial cells. This leaves a significant gap in accurately modeling the human tumor microenvironment, particularly when studying immunosuppressive mechanisms and therapy resistance.
Simpler Models: Insufficient for Complex Therapeutic Mechanisms
Monocultures of cancer cell lines, while failing to account for the intricate interactions between tumor cells and the surrounding tumor microenvironment, also lack tumor heterogeneity. The absence of stromal components in these models overlooks key factors influencing therapy mechanisms of action (MoA), particularly those targeting the tumor microenvironment. For example, therapies designed to modulate immune responses or disrupt fibroblast-mediated immune suppression are significantly affected by the presence and functionality of tumor microenvironment components. Consequently, these simplistic models often yield non-translatable results, leading to failure in clinical trials.
The Tumor Microenvironment's Role in Resistance, Recurrence, and Progression
The tumor microenvironment is a dynamic and interactive ecosystem that evolves with tumor progression. Specific elements of the tumor microenvironment, such as M2 macrophages and CAFs, actively promote resistance and recurrence by suppressing anti-tumor immunity and enhancing tumor survival. M2 Macrophages secrete IL-10, TGF-β, and VEGF, promoting immune evasion, angiogenesis, and tumor progression. CAFs can contribute to the desmoplastic reaction and produce extracellular matrix proteins, such as collagen, which act as physical barriers to therapy. They also release CXCL12 and TGF-β, further suppressing immune cell infiltration and activity.
Therapies targeting these immunosuppressive mechanisms have shown promise in preclinical settings but often fail in clinical trials due to the lack of a human-relevant tumor microenvironment in the models used for their development. To address these challenges, advanced ex-vivo co-culture models that mimic the human tumor microenvironment are essential. These models integrate multiple human cellular components, including tumor cells, immune cells, fibroblasts, and endothelial cells, in ratios and conditions that closely resemble specific tumor types.
Advantages of Ex Vivo Co-Culture Models
By using human cells for all tumor microenvironment components, these models eliminate the cross-species differences inherent in mouse models.
The proper characterization and ratios of human stromal cells enable accurate modeling of tumor microenvironment-driven mechanisms, such as immunosuppression and fibrosis. Real in-depth research is needed on the tumor microenvironment composition of different human tumors before starting to generate co-culture mimicking the tumor microenvironment.
To provide better translational relevance, it is ideal to leverage Patient Derived Xenograft-organoids (PDX-O) a valuable source of tumor cells that retain the heterogeneity and genetic complexity of the original tumor providing data that more closely predict clinical outcomes, reducing the high failure rate of therapies in clinical trials. Ultimately, using PDX-Os combined with human stromal and immune components in co-culture models creates a system that mirrors the patient-specific tumor microenvironment, enabling the evaluation of therapies in a clinically relevant context.
Applications of Ex Vivo Tumor Microenvironment Models: CAR-T Cell Therapy in Immunosuppressive Tumor Microenvironment
CAR-T cell therapy, a breakthrough in cancer immunotherapy, often struggles in solid tumors due to the immunosuppressive TME. M2 macrophages and CAFs inhibit CAR-T cell infiltration and activity through the secretion of TGF-β and CXCL12. Recent studies have demonstrated that anti-TGF-β antibodies or CXCR4 inhibitors can restore CAR-T cell functionality in ex-vivo co-culture models, highlighting the importance of these models for optimizing CAR-T therapeutics targeting CAFs [1]. Similarly, antifibrotic agents, such as inhibitors of lysyl oxidase (LOX) or TGF-β signaling, aim to disrupt the fibrotic stroma created by CAFs. Using ex vivo tumor microenvironment models, researchers have shown that these agents enhance the penetration and efficacy of chemotherapies and immunotherapies [2]. This highlights the key role these models can play in evaluating combination strategies targeting both the tumor and its microenvironment.
Developing Strategies to Mimic the Human Tumor Microenvironment
Creating robust ex-vivo tumor microenvironment models requires careful selection and characterization of human cells. Strategies include the selection of the right tumor microenvironment cells from the right origin, using the best E:T ratio between immune cells and patient-derived tumor cells, and defining optimal ratios of immune cells, fibroblasts, and endothelial cells to replicate a model-specific tumor microenvironment. In addition, functional validation is fundamental in ensuring that all cellular components behave as they do in vivo, including cytokine secretion and immune cell polarization. These considerations are critical for generating data that can effectively guide clinical decision-making.
Bridging the Gap to the Clinic
The development of human-relevant ex vivo co-culture models represents a significant step forward in cancer research. By faithfully replicating the human tumor microenvironment, these models provide a powerful platform for studying therapy resistance, optimizing treatment strategies, and improving the clinical translatability of preclinical findings. Ultimately, this approach aligns with the goal of delivering better outcomes for cancer patients.